The good, the bad, and the notable: COVID-19 information experiences
Rajesh Singh
Introduction. This study explores the COVID-19 information experiences of people at the outbreak of the pandemic in the United States.
Methods. The research data from 1,979 participants was collected through an online qualitative survey.
Analysis. A phenomenological approach was utilised to gain a deeper understanding of the COVID-19 information experiences. Cross tabulation was also used; however, the outcome is primarily qualitative.
Results. Three types of information experiences were identified, i.e., good, bad, and notable. The good information experiences indicated people’s appreciation for factual information, state government or local news, and information about the collective well-being of people. The bad information experiences illustrated people’s concerns about misinformation, fake news, and conspiracy theories, information coming from President Trump and his administration, health-related information, and information politics. The notable information experiences highlighted people’s positive outlook on information and their concerns about information uncertainty, the politics of information, and coronaphobia.
Conclusions. Findings suggest that information can significantly influence people’s feelings, moods, emotions, and experiences in polarising ways, and highlights implications for managing people’s well-being in times of mass misinformation and fake news.
DOI: https://doi.org/10.47989/irisic2222
Introduction
The COVID-19 pandemic created an infodemic, in which copious amounts of information, both accurate and inaccrate, rapidly spread through news and social media channels during a public health crisis (World Health Organization, 2020). As a result, people experienced information overload (Chae, et al., 2016; Rachfall, et al., 2015; Schommer, et al., 2001; Spira, 2011), widespread misinformation, and negative effects on their overall well-being (Liu, et al., 2021). Misinformation is a large part of information overload which was exacerbated by the COVID-19 pandemic. Misinformation regarding COVID-19 comes in many forms including conspiracy theories, rumors, lies, and disinformation (Dufva, 2020; Eysenbach, 2006; Ruokolainen and Widén, 2020; Wardle and Derakhshan, 2017). Popular cases of misinformation about COVID-19 included ‘the virus is a secret attempt by the global elite to reduce overpopulation, the virus is a bioweapon by the Chinese state to control the world, the virus is a plan by greedy big pharma firms to make money from vaccines’ (Nguyen and Catalan-Matamoros, 2020, p. 324). This misinformation was propagated by social media (Liu, et al., 2021; Matthes, et al., 2020), news outlets (Unger, 2018; Zhang, 2014), and even politicians (Hart, et al., 2020; Parmet and Paul, 2020; Schwartz, 2021). Consequently, this misinformation created uncertainty, confusing and misleading the public (Aghagoli, et al., 2020; Nguyen and Catalan-Matamoros, 2020). Major consequences result when people believe misinformation that could impact personal and public health and mental and emotional well-being.
Thus, the COVID-19 information crisis, exacerbated by media outlets and politicians, created a unique situation for studying how the information environment and socio-cultural context influence information experiences. This exploratory study seeks to understand people’s COVID-19 information experiences at the outbreak of the pandemic in the United States. The study provides some novel insights into information practices and experiences during crises and highlight implications for managing people’s well-being, especially when politicised information, misinformation and conspiracy theories are rampant in society.
Background
There are many different conceptualisations of information experiences. Generally, information experience is defined as ‘how people experience or derive meaning from the way in which they engage with information and their lived worlds as they go about their daily life and work’ (Bruce, et al., 2014, p. 6). Understanding people’s information experiences helps us understand people’s information behaviours, both how they interact with information sources and the effects that these information interactions have on their life and well-being (Shuva, 2020). Gorichanaz (2020) considers information experiences as the examination of human-information interactions at the moment of their unfolding. Savolainen (2019) emphasised the need to understand how embodied information relates to experiencing cognitive-affective information. Information experiences are contextual and help examine the human experience of information interactions (i.e., their perceptual, cognitive, and embodied experience contexts) by shedding light on the informational world (Hoyte, 2019; Lloyd, 2009; Soolhjoo, et al., 2022).
People have many information experiences and exhibit different information behaviour during times of crisis such as natural disasters and public health crises. Consequently, it is important to understand how people approach processing large quantities of information and its impact on affecting their overall well-being. The notion of well-being is a multifaceted concept. Existing conceptualisations consider happiness, a sense of purpose, wisdom, coherent philosophy of life, achievement, pleasure, and love as essential indicators of well-being (McMahan and Estes, 2011). An individual’s concept of well-being is subjective, depending on their life experiences and how they view them (Taylor, 2014). This means that information can significantly influence feelings, moods, and emotions differently, making people feel happy, angry, sad, panicked or accomplished, in addition to impacting their overall well-being.
During times of crisis, people seek and experience information differently when compared to less difficult times. Lund and Ma (2021) explored the behaviour of rural older adults, their coping mechanisms, and concerns with the health and political information they confronted during the COVID-19 pandemic. Montesi (2021) demonstrated sex differences in various dimensions of information behaviour and their implications for health outcomes. Zimmerman (2021) utilised information-horizons methodology to explore pre- and post-pandemic information seeking and emphasised the need for further research into health information-seeking behaviour in times of crisis. Furthermore, the COVID-19 infodemic triggered research about the impact of various online information sources including social media, official websites, online news sources, and search engines and their influence on people’s ability to process information and adopt preventive behaviour during pandemics (Farooq, et al., 2021). One of these studies showed that older people, in particular, determined their preventive strategies based on perceived information quality and threats through social media and adopted preventive behaviour including facemask-wearing, hand-washing, and social distancing (Nguyen and Le, 2021). Additionally, a qualitative study presented the views of Finnish respondents on information provision, relations/attitudes, emotions, societal impacts, and the evaluation of information at the time of the COVID-19 outbreak (Eriksson-Backa, 2020).
Excessive amounts of information can trigger feelings of distress, ambiguity, anxiety, and frustration due to a lack of suitable coping mechanisms contributing to negative perceptions and experiences (Swar, et al., 2017). Conversely, information overload can also positively impact well-being and cause some people to have positive and rewarding experiences by finding value in conflicting pieces of information, increased trust in information, and greater amounts of knowledge (Klausegger, et al., 2007). While some people reported negative experiences including fear and anxiety following the 9/11 terrorist attacks in the United States, others reported positive experiences including feelings of gratitude, interest, and love along with positive coping mechanisms which helped them remain resilient through hard times (Fredrickson, et al., 2003). Similarly, a study conducted by the Pew Research Center revealed how some people found silver linings despite the COVID-19 pandemic (Van Kessel, et al., 2021). People either deal with information overload by continuing to seek more information or completely avoiding information in favour of more positive and uplifting actions to manage their well-being. Lapatovska and Smiley (2014) discuss information behaviour during hurricane Sandy in 2012 that related to directly searching for problem-solving information, monitoring the storm’s progress, and passive information consumption. Throughout the different stages of the storm, people experienced information about physiological and safety needs, love, belonging, friendship, family, esteem or information that empowers, and self-actualisation via numerous media outlets. Thus, people found different ways of experiencing, interpreting, and interacting with information to understand and stay informed about the crisis. Similarly, Pang (2014) found that information seeking, especially about health information, increased during the Southeast Asian haze crisis in 2013 because information helps play a role in responding to crisis and alleviates anxiety in people directly impacted by the crisis.
Duggan and Banwell (2004) found, from investigating the dissemination of information during a suspected tuberculosis incident, that effective dissemination of information during a crisis requires targeting information to specific audiences in the community, persuasion by leaders in the community, and a willingness by recipients to accept new knowledge. Two barriers to disseminating information during crises are assumptions made by information providers about their audience and ‘the need for homophilous communication’ in which communication is more effective when individuals share similar characteristics and attributes (Duggan and Banwell, 2004). Moreno, et al. (2020) found that, during the COVID-19 crisis in Spain, information seeking was greatly impacted because ‘the choice of medium influences the public’s sense-making of the crisis and moderates their acceptance of crisis messages’ (2020), p.11). A recent study explored information practices, experiences, and coping mechanisms of young adults in managing COVID-19 related information across two diverse information environments and socio-cultural contexts in Finland and the US; it highlights similarities in the approaches and coping mechanisms young people use to manage their emotional well-being in addition to reporting considerable variations in their perceptions about the role of media and politics in shaping how pandemic-related information was consumed and evaluated (Karim, et al., (2021).
Against this backdrop, this study seeks to gain a deeper understanding of people’s information consumption habits, information handling approaches, and COVID-19 information experiences at the outbreak of the pandemic in the United States.
Methods
A qualitative survey was circulated between May 5 and June 4, 2020, in the U.S. (Appendix 4). The survey asked mostly open-ended questions to develop an understanding of the roles that information and emotion play during a crisis and to identify strategies for managing information and media consumption. Additionally, the survey inquired about the information sources that people used to search for information about COVID-19 and sought to understand how they evaluated the information’s reliability. The rationale behind conducting a qualitative survey was to capture raw emotions of people’s information experiences as they unfolded during the pandemic. This study focuses on understanding the information experiences of respondents based on responses to the following open-ended questions:
- Please share 1-2 examples of good experiences and 1-2 examples of bad experiences that you’ve had regarding information about the coronavirus pandemic.
- Please share any other notable experiences regarding coronavirus information in general.
Data collection and analysis approach
The survey was distributed online through various online channels including listserv, social media, and Facebook groups. The survey targeted people with varied backgrounds and geographical locations; respondents included librarians, information professionals, archivists, lawyers, accountants, teachers, pastors, and students. Additionally, an appeal was made to the survey participants to pass on the survey link to others interested in responding.
This study utilised a phenomenological approach to gain a deeper understanding of the information experiences of people as they navigated pandemic-related information. Respondents’ comments were analysed utilising a phenomenological approach that follows Van Manen’s (1990), p.79) proposal that ‘themes may be understood as the structures of experience’. Effort was made to uncover experiences informing telling, meaningful, and thematic expressions in respondents’ perceptions of pandemic-related information. Prior information behaviour studies have also utilised a similar phenomenological approach in understanding information experiences (Yates, 2015; Yates, Partridge and Bruce, 2012).
In addition, cross tabulation was also used to pinpoint relationships between respondents’ information experiences and demographic variables in SPSS. However, the outcome of the study remains primarily qualitative.
Participants’ characteristics
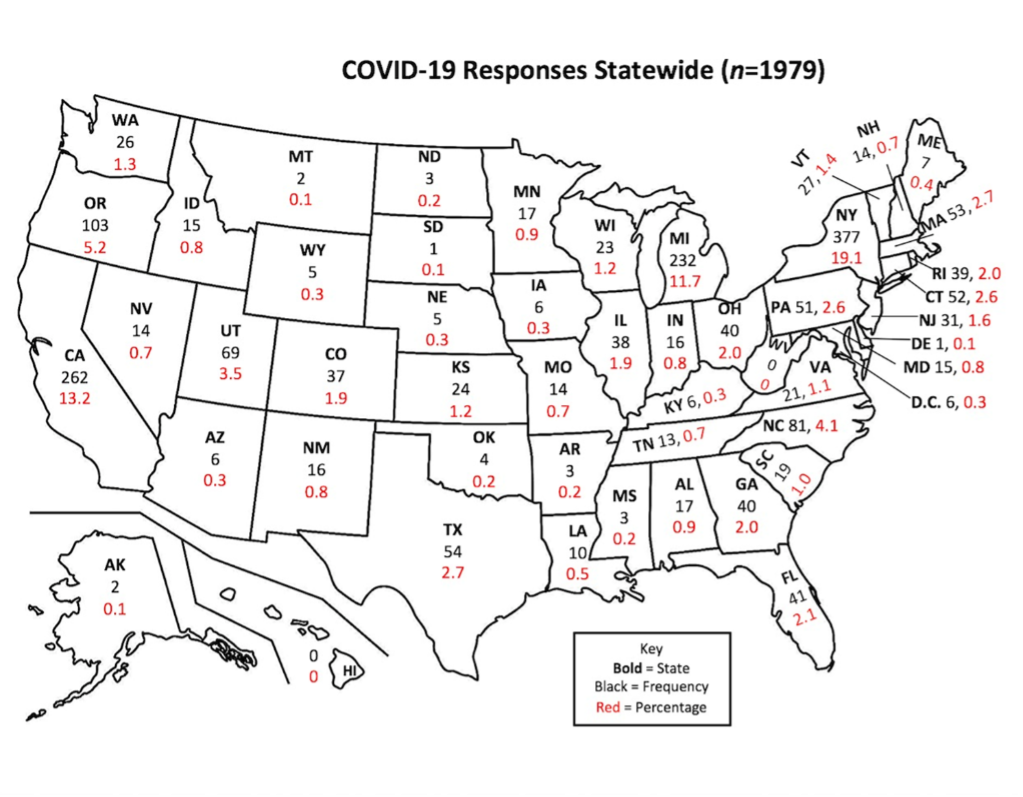
The sample included 1.979 participants from various geographical regions including 48 states and Washington, D.C.; the majority of the respondents were from New York (19.1%), California (13.2%), and Michigan (11.7%). Figure 1 displays the geographical coverage of the sample.
The respondents represented various age groups ranging from 18-88 years old. Respondents were overwhelmingly female (82.9%); males accounted for 14.3% of the sample, while 2.8% of participants identified as non-binary, or did not wish to disclose their gender. While most respondents were employed (83.4%), a relatively small number of participants reported as self-employed (3.9%), unemployed (2.2%), retired (8.5%), homemaker (3.2%), or veteran (1.4%). A small percentage of respondents (10.7%) were either students and/or belonged to the categories indicated above. The analysis reveals that 6.6% of respondents were either diagnosed with COVID-19 or knew someone in their immediate environment who received a positive diagnosis. Lastly, 37.1% of respondents indicated that they belonged to a group considered at high risk for severe COVID-19 infection. Table 1 displays the demographic composition of the sample.
| Variables | Frequency (%) |
|---|---|
| Age> | |
| 18-29 | 154(7.8%) | 30-39 | 406 (20.5%) | 40-49 | 433 (21.9%) |
| 50-59 | 468 (23.6%) |
| 60-69 | 365 (18.4%) |
| 70-79 | 114 (5.8%) |
| 80-88 | 12 (0.6%) |
| Undisclosed | 27 (1.4%) |
| Gender | |
| Male | 283 (14.3%) | Female | 1641 (82.9%) | Undisclosed/non-binary | 55 (2.8%) |
| Occupational status | |
| Employed | 1651 (83.4%) | Self-employed | 77 (3.9%) | Unemployed | 44 (2.2%) |
| Homemaker | 63 (3.2%) |
| Retired | 168 (8.5%) |
| Veteran | 28 (1.4%) |
| Students and/or belonged to the above categories |
211 (10.7%) |
| COVID-19 high risk group status | |
| Yes | 735 (37.1%) | No | 1091 (55.1%) | Don’t know | 153 (7.7%) |
| COVID-19 Diagnosed/Knew COVID-19 Infected Person in their Immediate Environment |
|
| Yes | 130 (6.6%) | No | 1771 (89.5%) | Don’t know | 78 (3.9%) |
The analysis identified three different information experiences, i.e., good, bad, and notable. A brief overview of the themes which emerged is presented below in Figure 2.
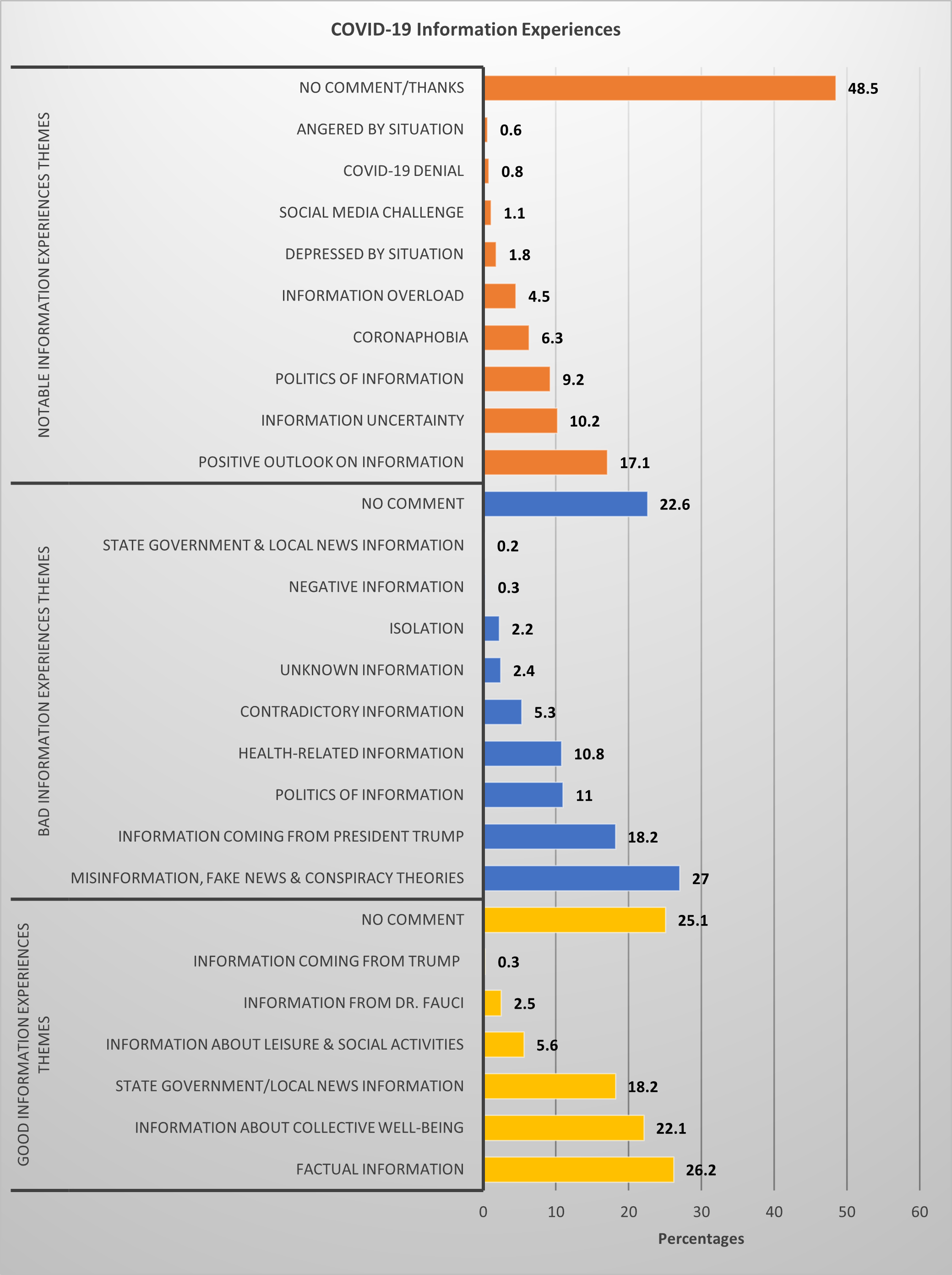
Figure 2: Themes in the good, bad, and notable information experiences
Findings
Good information experiences
A substantial number of respondents (26.2%) identified receiving factual information about the pandemic, such as social distancing, handwashing and mask-wearing, from reputable organisations (e.g., CDC, WHO), their preferred media outlets (e.g., radio, TV), hospitals, the internet and employers as predominantly good experiences. They appreciated the quality, accuracy and speed of the information they received from their preferred sources and found them helpful when making informed decisions. Moreover, they also appreciated the efforts of these authoritative organisations in alerting people about the possibility of information manipulation and fabrication. They found accurate, credible and evidence-based information helpful in fulfilling their information needs and managing their physical and emotional well-being. The analysis revealed that most appreciation for factual information came from participants aged 50–59, 40–49, 30–39, and 60–69 years (Table 2). Additionally, participants from employed (83.4%), student (12.1%) and retired (8.5%) groups demonstrated a higher appreciation for factual information.
A significant number of respondents (22.1%) found information about collective well-being encouraging and refreshing. The most appreciation for this type of information came from participants aged 50–59 years, followed by 30–39, 60–69, and 40–49 years (Table 2). Furthermore, participants from the employed (84%), student (9.4%) and retired (6.9%) groups appeared to be more appreciative of information about collective well-being. These groups enjoyed reading uplifting stories about people helping each other and sharing resources, and their recovery and coping mechanisms. Interestingly, some respondents appeared to envision a bright, optimistic and hopeful future based on news regarding COVID-19 survival, pandemic management progress in other countries, possible vaccines, the heroism of health care workers, flattening the curve and decreasing pollution levels.
A substantial number of participants (18.2%) found their state governments’ news briefings and televised announcements helpful and informative and appeared to be pleased with their information distribution approach during the pandemic. Table 2 shows that a majority of these participants belonged to those aged 30–39, 40–49, 50–59, and 60–69 years. They were primarily employed (85%) and students and/or belonged to other occupational groups (5.8%).
As information environment changed at the outbreak of the pandemic, some respondents (5.6%) appreciated the opportunity to engage in leisure and social activities that provided the flexibility to work from home, allowing them more time with their friends, relatives, and pets. Additionally, they were thankful for the downtime and enjoyed reading, exercising, watching funny videos and other leisure and social activities while working from home. A substantial number of these participants were 50–59 years, followed by 30–39, 40–49, and 60–69 years. It is important to note that many people considered spending time with friends and family as a leisure activity. They associated social activities with physically being in the same space as their immediate household, unlike others who increased their socialisation with outside friends and family through technology, such as emails, phone calls and Zoom video conferencing. Similarly, some people enjoyed information on Facebook group on ‘coping with covid19’ fun posts and images , in addition to others who binge-watched Netflix as their leisure activity.
Overall, the analysis highlighted a significance tendency (df = 36; p = .002) where good information experiences were cross-tabulated across various age groups (Table 2).
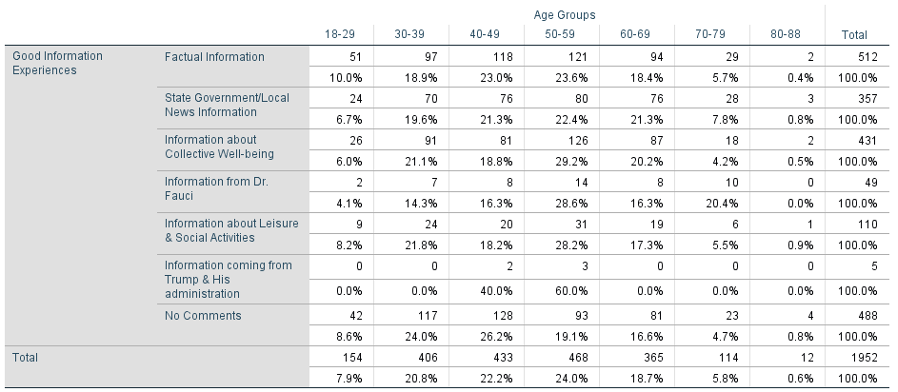
Table 2. Good information experiences across various age groups
df = 36 ; p = 0.002
Good information experiences highlighted a significance tendency among retired participants (df = 6; p = .020). A retired participant’s comment highlights her appreciation for factual information: ‘I appreciated a retired nurse in my network sharing ways to stay safe and other resources like available take out options’. Overall, most of retired participants demonstrated their appreciation for state government and local news information, factual evidence, news regarding the collective well-being and information from Dr Fauci. Additionally, good information experiences indicated a significance tendency among students (df = 6; p = .003). A substantial number of students highlighted their appreciation for receiving information from their state government and local news distribution sources, factual evidence, news regarding collective well-being and opportunities to engage in social and leisure activities. A student commented about the usefulness of factual and helpful information:
‘There have been several videos shares on social media by people in the healthcare industry talking about their experiences and how this is not like the flu. I can't say I enjoyed watching those, but I felt they were very informative and more informative than what we see or read in the news’.
Similarly, another student appreciated receiving information about the collective well-being:
‘During this time, people are sincerely reaching out to support each other and trying their best to share useful information. They are also using social media and video conferencing to support and constructively teach and entertain each other’.
Participants who were at high risk of COVID-19 across Yes, No, and Don’t Know groups appreciated receiving factual information from their preferred authoritative sources, found local/state news briefings informative, praised information about collective well-being and valued Dr Anthony Fauci for providing trusted, credible and scientific information about the pandemic. Overall, good information experiences indicated a significance tendency (df = 6; p = .080) regarding participants with a high-risk COVID-19 status (Table 3).
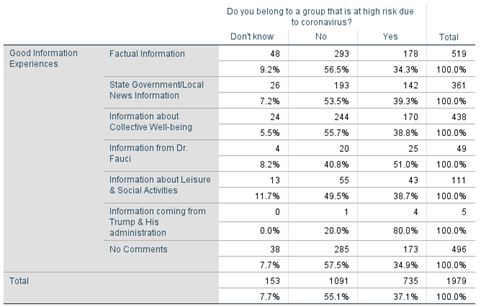
Table 3: Good information experiences across COVID-19 high-risk group participants
df = 6 ; p = 0.080
Overall, participants used phrases such as pleased, helpful, safe, encouraging and calm , among others, to characterise their good information experiences. Good information experiences indicated an appreciation for factual information, state government or local news and information about the collective well-being. A summary highlighting the major themes of good information experiences and their representative comments are given below in Appendix 1.
Bad information experiences
Bad information experiences primarily comprised of a constant circulation of misinformation, fake news and conspiracy theories (27%), information coming from President Trump and his administration (18.2%) and information politics (11%). These three themes appeared to be seemingly connected and posed significant challenges for people when navigating health-related information (10.8%). Furthermore, people were angry with their friends, family and the media for spreading fabricated and unreliable information on the internet and social media outlets. Most of these participants belonged to the 50–59, 40–49, and 30–39 age groups (Table 4).
A significant number of respondents (18.2%) found information originating from President Trump and his administration to be problematic. They characterised the President’s briefings as toxic, uninformed and dangerous and found the information unhelpful for their well-being. The biggest criticism came from participants aged 60–69, followed by those aged 50–59, 40–49, and 30–39. Interestingly, some respondents (11%) blamed politicians for twisting information about the number of ventilators and N95 masks. They also thought media outlets were fearmongering by showing overcrowded hospitals and predicting high death rates. These participants were primarily from the 60–69, 50–59, 30–39, and 40–49 age groups and raised concerns about information politics from some politicians, the media and organisations. Overall, Table 4 shows that bad information experiences indicated the strongest significance level across the various age groups (df = 54; p =.000).
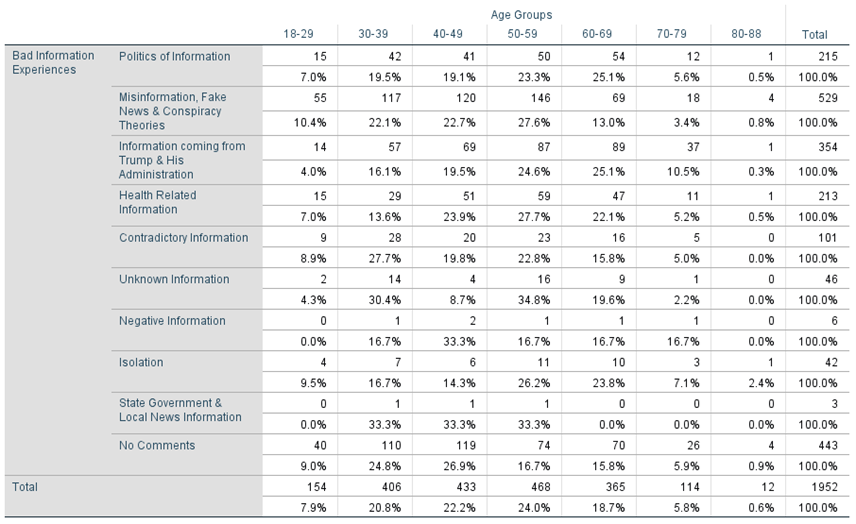
Table 4. Bad information experiences across various age groups
df = 54 ; p = 0.000
Some respondents (10.8%) highlighted that negative or misleading news stories about health-related information affected their emotional well-being. They also raised concerns about people disregarding social distancing guidelines. Respondents (5.3%) also reported contradictory information as problematic and alluded to quickly changing guidelines regarding shops, masks, social distancing, and stay-at-home orders. A small number of respondents (2.4%) were concerned about the unknown nature of the COVID-19 virus and its transmission, inadequate news coverage about recoveries and the lack of research results; some appeared to be concerned about the lack of useful supplies, such as toilet paper, sanitisers and soaps. Similarly, a handful of respondents reported that isolation had a significant effect on their emotional well-being during the COVID-19 crisis. A small number of respondents (0.3%) blamed media outlets for their negative information coverage, while others (0.2%) were critical of the information distribution approach of their state government.
Bad information experiences highlighted a significance tendency among homemakers (df = 9; p = .014). A homemaker shared her sentiments about misinformation and its negative ramifications: ‘I don't like fear mongering stories and hysteria in my mom groups who are hungry for info’. Overall, homemakers’ major concerns included the constant stream of misinformation, information coming from President Trump and his administration, contradictory or health-related information, the politics of information and isolation. Additionally, bad information experiences indicated a significance tendency among retired participants (df = 9; p = .026). A retired participant expressed her concerns about information coming from President Trump: ‘I have watched a few daily briefings by the President. They are confusing and distracting. No help at all’. Overall, a substantial number of retired participants raised major concerns about the information coming from President Trump and his administration, the constant flow of misinformation and the politics of information.
Overall, bad information experiences indicated a significance tendency (df = 18; p = .011) among participants with high-risk COVID-19 status across the Yes, No, and Don’t Know groups (Table 5). The findings indicate that the participants’ bad information experiences vary over this issue. The Yes and No participants raised quite similar concerns about information politics (Yes = 46.3%; No = 45.4%) and information coming from President Trump and his administration (Yes = 44%; No = 49.3%). Furthermore, while the Yes and No groups were troubled by the constant circulation of fake news, misinformation, conspiracy theories, and health-related or contradictory information, their concerns varied on these issues.
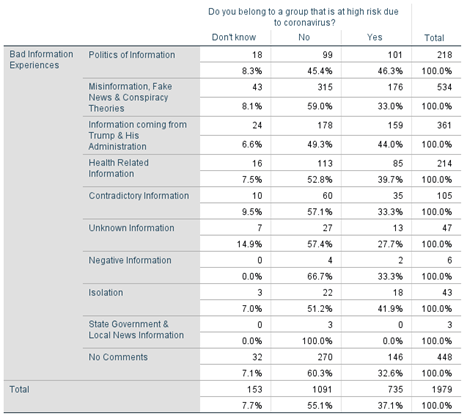
Table 5. Bad information experiences across high COVID-19 risk status groups
df = 18 ; p = 0.011
Similarly, the analysis highlighted a significance level (df = 18; p = .025) across the Yes, No or Don’t know groups when bad information experiences were cross-tabulated with the variable that asked if participants were either infected with COVID-19 or knew someone in their immediate environment who had a confirmed COVID-19 infection (Table 6). Participants raised concerns about the constant circulation of misinformation, fake news and conspiracy theories, information politics, information coming from Trump and his administration and contradictory information in general. Additionally, participants from the Yes and Don’t know groups appeared to be equally troubled by isolation due to COVID-19 stay-at-home orders.
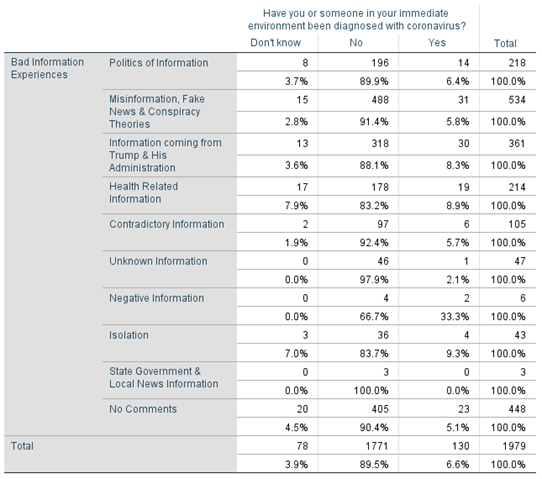
Table 6. COVID-19 diagnosed/knew COVID-19 infected person in their immediate environment
df = 18 ; p = 0.025
Overall, participants expressed phrases such as shocked, panicked, frustrated, angered, depressed or similar strong expressions to characterise their bad information experiences. Bad information experiences illustrated concerns about misinformation, fake news and conspiracy theories, information coming from President Trump and his administration, health-related information, and information politics. A summary highlighting the major themes of bad information experiences and their representative comments are given below in Appendix 2.
Notable information experiences
Notable information experiences can be understood as the interaction between pandemic-related events and personal memories that made them feel good, bad, sad, shocked or angered, or evoked similar strong emotions. As part of their notable information experiences, participants either expressed novel events or considered it worth reiterating some of their good or bad experiences.
The analysis revealed some interesting themes about respondents’ notable information experiences during the COVID-19 pandemic. Out of the 51.1% respondents who shared their notable information experiences, 17.1% of them highlighted a positive outlook for information. Despite challenging circumstances, these respondents were able to find positivity by reading scientific information from credible and reputable sources, working from home, exercising more and engaging in leisure activities. Some respondents (10.1%) highlighted information uncertainty as one of their notable experiences. Conflicting information included the evolving research about the COVID-19 virus, lab tests, vaccines, herd immunity and disagreements between politicians and the scientific community. Furthermore, some respondents (8.8%) raised concerns about information politics and blamed politicians and the media for fabricating COVID-19-related information for political gain. About 6.8% of respondents perceived the COVID-19 virus as dangerous, placing them in the coronaphobia category. These respondents were fearful about going to grocery stores and were troubled by the lack of mask-wearing and social distancing by others, causing them to avoid socialising with friends and relatives. A small number of respondents (4.5%) indicated information overload as a notable experience and alluded to information addiction across various media outlets. A handful of respondents expressed feelings of depression (1.8%), characterised social media as both a blessing and a curse (1.1%), were astounded by COVID-19 denial (0.8%) and were angered by the overall situation (0.6%) due to staying at home, price extortion by some grocery stores, lack of supplies and public paranoia.
Overall, notable information experiences highlighted people’s positive outlook on information and their concerns about information uncertainty, the politics of information, and coronaphobia. A summary highlighting the major themes of notable information experiences and their representative comments are given below in Appendix 3.
Discussion
Different life events may impact a person’s information experiences as well as their information behaviour. The COVID-19 pandemic created a unique information crisis in the form of an infodemic, in which vast quantities of information, both accurate and inaccurate, were disseminated across various media platforms (World Health Organization, 2020). This research explored participants’ COVID-19-related information experiences during the stay-at-home orders. Good, bad, and notable information experiences emerged.
Bad COVID-19 information experiences included the circulation of misinformation, fake news and conspiracy theories as participants’ major concerns. People appeared to be frustrated with their friends, family and distant relatives who shared misinformation, conspiracy theories, half-truths from unreliable sources, disinformation and sensational news and videos through social media outlets, such as Facebook and Instagram. Even though social media acted as a platform for sharing information experiences, it was also a vehicle for disseminating falsehoods, misinformation and contradictory information concerning COVID-19. Furthermore, the information provided by President Trump and his administration exacerbated this problem. Consequently, these socio-cultural factors created a unique situation of information politics that included information withholding as well as the dissemination of misleading information, contradictory information, misinformation, disinformation, and conspiracy theories. Many people identified information politics as one of their bad and notable experiences, criticising both politicians and the media for amplifying the politicisation and polarisation of COVID-19 information, exacerbating partisan divides and jeopardising public health. Additionally, isolation, frequently changing guidelines about mask-wearing and information uncertainty due to constantly evolving novel information about the virus contributed to information fatigue and information anxiety (Soroya, et al., 2021). Consequently, this information crisis caused people to actively seek more information to better understand the situation. However, locating factual, credible, and reliable health-related information to manage well-being remained challenging in the COVID-19 information crisis. Nonetheless, the participants’ good and notable information experiences revealed that factual, accurate and uplifting information about the pandemic helped people manage their physical and emotional well-being by instilling feelings of confidence, hope, optimism, and resiliency.
Findings suggest that participants’ good information experiences included phrases such as pleased, helpful, safe, encouraging and calm , among others. Conversely, participants expressed phrases such as shocked, panicked, frustrated, angered, depressed , or similar strong expressions, in their bad information experiences. The contrast between these two types of information experiences suggests that information can significantly influence people’s feelings, moods, and emotions in polarising ways. In addition, it can impact their overall well-being positively or negatively, especially when they are inundated with a stream of both accurate and inaccurate information in a crisis. For the people encountering these large quantities of information, an information crisis can influence their overall well-being. While there is no single definition of well-being, the Centres for Disease Control and Prevention (2018) regard it as the presence of positive emotions and moods (e.g., contentment, happiness), the absence of negative emotions (e.g., depression, anxiety), satisfaction with life, fulfilment, and positive functioning, and views physical and mental well-being as essential to overall well-being in terms of public health. While it may be neither a good strategy nor a solution to avoid negative information, it should be possible to provide accurate and credible information about the crises as well as suitable coping approaches, which would help to enhance individual and collective well-being in society.
A substantial number of participants highlighted their appreciation for reading stories and information about the collective well-being of society. They also indicated that the opportunity to engage in leisure and social activities outdoors and indoors with friends, family, colleagues, and acquaintances positively impacted their overall well-being. Their comments suggest that information about the collective well-being of society helped them stay positive and calm, and to cope and recover during the pandemic. Similar findings were reported in a study conducted by the Pew Research Centre, revealing how some people found positivity, despite the COVID-19 information crisis (Van Kessel et al., 2021). It would be beneficial to understand how information interacts with the emotional, cognitive, behavioural, personality and contextual components of well-being, hope and optimism in uncertain and adverse situations and its impact on well-being (Bruininks and Howington, 2019).
As discussed earlier, participants’ highlighted information politics as one of their bad and notable experiences. While a handful of respondents found information coming from President Trump and his administration helpful, the majority appeared to be troubled by the administration’s quality of information. Additionally, participants were critical of public officials, politicians, the media, and the public for twisting, manipulating and politicising information. Consequently, this politicisation of COVID-19 information created different narratives, depending on how people viewed the information (and misinformation) that was either shared or withheld, in addition to impacting their overall well-being. Studying the political dimension and its influence on information quality would be a worthy area of research in future health crises, especially when people are not privy to all political information or do not understand the political information that is presented to them. Subsequently, this could have an impact on their ability to navigate health-related information, manage their physical and emotional well-being, and be engaged citizens.
Participants’ information experiences also highlighted how media reports affected their perceptions about the COVID-19 crisis and their overall well-being within it. Additionally, these findings revealed an increasing distrust of the media, especially due to the mass misinformation and fake news of recent times. This suggests that the media needs to be careful when handling, monitoring and disseminating information about a crisis. People enjoyed seeing others’ stories and valued the knowledge that they had shared experiences with others. Social media can be a valuable tool to communicate information in real-time, identify important situational information that may be of value to different groups of people, and identify needs in a particular region (Ghosh, et al., 2018). Page, et al. (2013) found that best practices for social media use included ‘integration of multimedia and links into updates’, ‘proper use of hashtags and tagged keywords’ and a ‘balance between official and conversational updates’ (2013), p. 25). These practices can be used by both traditional news outlets and government agencies when disseminating crisis information and media reports on social media platforms. However, media, political and information landscapes vary across the United States, European and Nordic countries (Iyengar, et al., 2010); Karim, et al., 2021). Further research would be helpful to better understand the media differences between the United States and other countries, so effective media communication strategies can be developed to help people manage their well-being in times of crisis.
An extensive effort was undertaken to complete this research; however, several limitations could not be avoided. Despite the large sample, the qualitative nature of this study presents constraints in generalising its findings concerning how people navigated and processed COVID-19 pandemic-related information. Despite cross-tabulations indicating a significance tendency between participants’ information experiences and some demographic variables, it is difficult to have confidence in the findings. Another limitation of this study is that all the survey responses were self-reported and, therefore, may be biased. The potential for bias was clear in respondents’ comments in both the bad and notable information experiences groups. Nevertheless, the research findings provide some novel insights into information practices and experiences during crises and highlight implications for managing the population’s overall well-being, especially when politicised information, misinformation and conspiracy theories are rampant in society.
Conclusion
This exploratory study highlights how people engaged with information as it unfolded at the outbreak of the COVID-19 information crises during the stay-at-home orders. It highlights the importance of factual, accurate and uplifting information and the positive effect of this on people’s physical and emotional well-being in crises. Conversely, a constant flow of misinformation, negative and conflicting stories and politicisation of information have a negative impact on a person’s well-being. Findings suggest that information can significantly influence people’s experiences in polarising ways and highlights implications for managing people’s overall physical and emotional well-being in times of mass misinformation and fake news. Further exploration into the role of information on a population’s overall physical and emotional well-being may potentially be helpful to minimise bad information experiences and expand understanding of well-being and positive human functioning. Additionally, the findings can be applied when planning effective information campaigns, health information policies and media communication strategies to help people employ effective processes to manage information during a crisis.
About the author
Rajesh Singh is an Associate Professor in the Division of Library and Information Science, St. John’s University, New York. He received his Ph.D. in Information Studies from the Department of Information Studies, Åbo Akademi University, Finland. He can be contacted at singhr1@stjohns.edu.
References
- Aghagoli, G., Siff, E.J., Tillman, A., & Feller, E.R. (2020).OVID-19: misinformation can kill. Rhode Island Medical Journal, 103(5), 12-14. PMID: 32481773
- Bruininks, P., & Howington, D. E. (2019). Hopul + hoping = hope: unique experiential features in the measurement of emotion. The Journal of Positive Psychology, 14(3), 341-353. https://doi.org/10.1080/17439760.2018.1437465
- Bruce, C., Davis, K., Hughes, H., Partridge, H., & Stoodley, I. (2014). In C. Bruce, K. Davis, H. Hughes, H. Partridge, & I. Stoodley, (Eds.), Information experience: approaches to theory and practice. Information experience: contemporary perspectives, (pp. 5-15). Emerald Group Publishing Limited. https://doi.org/10.1108/S1876-056220140000010001
- Chae, J., Lee, C. J., & Jensen, J. D. (2016). Health Communication, 31(5), 626-634. (https://doi.org/10.1080/10410236.2014.986026
- Centers for Disease Control and Prevention. (2018, October 31). Well-being concepts. Centers for Disease Control and Prevention https://www.cdc.gov/hrqol/wellbeing.htm (Internet Archive)
- Dufva, M. (2020). Megatrendit 2020. SITRA. https://www.sitra.fi/app/uploads/2019/12/megatrendit-2020.pdf (Internet Archive)
- Duggan, F., & Banwell, L. (2004). Constructing a model of effective information dissemination in a crisis. Information Research, 9(3). http://informationr.net/ir/9-3/paper178.html (Internet Archive)
- Eriksson-Backa, K. (2020). Views on Covid-19 information. Informaatiotutkimus, 39(2-3), 54-59. https://journal.fi/inf/article/view/98616/56754 (Internet Archive)
- Eysenbach, G. (2006). Infodemiology: Tracking flu-related searches on the web for syndromic surveillance. AMIA 2006 Symposium Proceedings. 244-248. https://journal.fi/inf/article/view/98616/56754. PMCID: PMC1839505.
- Farooq A., Laato, S., Najmul Islam, A.K.M., & Isoaho, J. (2021). Understanding the impact of information sources on COVID-19 related preventive measures in Finland. Technology in Society, 65(101573). https://doi.org/10.1016/j.techsoc.2021.101573
- Fredrickson, B. L., Tugade, M. M., Waugh, C. E., & Larkin, G. R. (2003). What good are positive emotions in crisis? A prospective study of resilience and emotions following the terrorist attacks on the United States on September 11th, 2001. Journal of Personality and Social Psychology, 84(2), 365–376. https://insidehighered.com/news/2020/04/21/early-journal-submission-data-suggest-covid-19-tanking-womens-research-productivity. PMID: 12585810
- Ghosh, S., Ghosh, K., Ganguly, D., Chakraborty, T., Jones, G.J.F., Moens, M.F., & Imran, M. (2018). Exploitation of social media for emergency relief and preparedness: recent research and trends. Information Systems Frontiers, 20(5), 901-907. https://doi.org/10.1007/s10796-018-9878-z
- Gorichanaz, T. (2020). Information experience in theory and design. Emerald Group Publishing.
- Hart, P. S., Chinn, S., & Soroka, S. (2020). Politicization and polarization in COVID-19 news coverage. Science Communication, 42(5), 679-697. https://doi.org/10.1177/1075547020950735
- Hoyte, P. (2019). & Hicks, A. (2021). Implications of the embodied, enactive mind on theorizing about information experience. In Proceedings of the Association for Information Science and Technology, 56(1), 413-416. https://doi.org/10.1002/pra2.40
- Iyengar, S., Curran, J., Brink Lund, A., Salovaara-Moring, I., Hahn, K. S., & Coen, S. (2010). ross-national versus individual-level differences in political information: a media systems perspective. Journal of Elections, Public Opinion and Parties, 20(3), 291-309. https://doi.org/10.1080/17457289.2010.490707
- Karim, M., Singh, R., & Widen, G. (2021). Dealing with the COVID-19 infodemic: understanding young people’s emotions and coping mechanisms in Finland and the United States. Nordic Journal of Library and Information Studies, 2.(1). https://doi.org/10.7146/njlis.v2i1.125220
- Klausegger, C., Sinkovics, R. R., & Zou, H. J. (2007). Information overload: a cross-national investigation of influence factors and effects. Marketing Intelligence & Planning, 25 (7), 691–718. https://doi.org/10.1108/02634500710834179
- Lapatovska, I. & Smiley, B. (2014). Proposed model of information behaviour in crisis: the case of Hurricane Sandy. Information Research, 19(1), paper 610, 691–718. http://InformationR.net/ir/19-1/paper610.html (Internet Archive)
- Liu, H., Liu, W., Yoganathan, V., & Osburg, V.S. (2021). COVID-19 information overload and generation Z’s social media discontinuance intention during the pandemic lockdown. Technological Forecasting and Social Change, 166 https://doi.org/10.1016/j.techfore.2021.120600
- Lloyd, A. (2009). Informing practice: information experiences of ambulance officers in training and on-road practice.. Journal of Documentation, 65(3), 396-419.https://doi.org/10.1108/00220410910952401
- Lund, B., & Ma, J. (2021). Exploring information seeking of rural older adults during the COVID-19 pandemic. Journal of Information Management, 74(1), 54-77. https://doi.org/10.1108/AJIM-04-2021-0118
- Matthes, J., Karsay, K., Schmuck, D., & Stevic, A. (2020). “Too much to handle”: impact of mobile social networking sites on information overload, depressive symptoms, and well-being. Computers in Human Behavior, 105, >1-11. https://doi.org/10.1016/j.chb.2019.106217
- Montesi, M. (2021). Gender differences in information behavior during the Covid-19 health crisis in Spain. LIS.it, 12, 73-87. https://doi.org/10.4403/jlis.it-12698
- Moreno, A., Fuentes-Lara, C., & Navarro, C. (2020). Covid-19 communication management in Spain: exploring the effect of information-seeking behavior and message reception in public’s evaluation. El professional de la información, 29(4), 1-16. https://doi.org/10.3145/epi.2020.jul.021
- Nguyen, A., & Catalan-Matamoros, D. (2020). Digital mis/disinformation and public engagement with health and science controversies: Fresh perspectives from Covid-19. Media and Communication, 8(2), 323-328. https://doi.org/10.17645/mac.v8i2.3352
- Nguyen, T. H., & Le, X. C. (2021). How social media fosters the elders’ COVID-19 preventive behaviors: perspectives of information value and perceived threat. Library Hi Tech, 39(2), 776-795. https://doi.org/10.1108/LHT-09-2020-0241
- Page, S., Freberg, K., & Saling, K. (2013). Emerging media crisis value model : a comparison of relevant, timely message strategies for emergency events. Journal of Strategic Security, 6, 20-31.https://doi.org/10.5038/1944-0472.6.2.2
- Pang, N. (2014). Crisis-based information seeking: monitoring versus blunting in the information seeking behaviour of working students during the Southeast Asian Haze Crisis. In Proceedings of ISIC, the Information Behaviour Conference, Leeds, September 2-5, 2014: Part 1(6), paper isic14. http://InformationR.net/ir/19-4/isic/isic14.html (Inernet Archive)
- Parmet, W., & Paul, J. (2020). COVID-19: the first posttruth pandemic. American Journal of Public Health, 110(7), 945-946. https://doi.org/10.2105/AJPH.2020.305721
- Rachfall, T., Förster-Trallo, D., Williamson, E., & Temple, B. (2015). The impact of information overload on individual stress feelings of management accountants [Conference paper]. International Academic Conference on Management, Economics and Marketing, Budapest. https://bit.ly/3dSLURf
- Ruokolainen, H., & Widén, G. (2020). Conceptualising misinformation in the context of asylum seekers. Information Processing & Management, 57(3), 102127. https://doi.org/10.1016/j.ipm.2019.102127
- Savolainen, R. (2019). Elaborating the sensory and cognitive-affective aspects of information experience. Journal of Librarianship and Information Science, 52(3), 671-684.https://doi.org/10.1177/0961000619871595
- Schommer, J. C., Doucette, W. R., & Worley, M. M. (2001). Processing prescription drug information under different conditions of presentation. Patient Education and Counseling, 43(1), 49-59. https://doi.org/ 10.1016/s0738-3991(00)00145-2
- Schwartz, M. S. (2021, February 15). New York governor defends temporarily withholding nursing home coronavirus data. NPR. https://www.npr.org/2021/02/15/968199651/new-york-governor-defends-temporarily-withholding-nursing-home-coronavirus-data (Internet Archive)
- Shuva, N. Z. (2020). Information experiences of Bangladeshi immigrants in Canada. Journal of Documentation, 77(2), 479-500. https://doi.org/10.1108/JD-08-2020-0137
- Soolhjoo, N., Krtalic, M. & Goulding, A. (2022). Pets and people. Information experience of multispecis families. Journal of Documentation, 78 (5), 1092-1108. https://doi.org/10.1108/JD-03-2021-0052
- Soroya, S. H., Farooq, A., Mahmood, K., Isoaho, J., & Zara, S. E. (2021). From information seeking to information avoidance: understanding the health information behavior during a global health crisis. Information Processing & Management, 58 (2), 102440. https://doi.org/10.1016/j.ipm.2020.102440
- Spira, J. (2011). Information overload: none are immune. Information Management, 21(5), 32.
- Swar, B., Hameed, T., & Reychav, I. (2017). Information overload, psychological ill-being, and behavioral intention to continue online healthcare information search. Computers in Human Behavior, 70(5), 416-425. https://doi.org/10.1016/j.chb.2016.12.068
- Unger, D.C. (2018). US news media under pressure: then and now. The SAIS Review of International Affairs, 38(2), 5-14. https://doi.org/10.1353/sais.2018.0011
- Van Kessel, P., Baronavski, C., Scheller, A., & Smith, A. (2021, March 5). In their own words, Americans describe the struggles and silver linings of the COVID-19 pandemic. Pew Research Center. https://www.pewresearch.org/2021/03/05/in-their-own-words-americans-describe-the-struggles-and-silver-linings-of-the-covid-19-pandemic/ (Inernet Archive)
- Van Manen, M. (1990). Researching lived experience: human science for an action sensitive pedagogy. State University of New York Press. 77-110.
- World Health Organization. (2020). Infodemic. https://www.who.int/health-^topics/infodemic#tab=tab_1 (Internet Archive)
- Yates, C. (2015). Exploring variation in the ways of experiencing health information literacy: A phenomenographic study. Library & Information Science Research, 37(3), 220-227. https://doi.org/10.1016/j.lisr.2015.04.003
- Yates, C., Partridge, H. L., & Bruce, C. S. (2012). Exploring information experiences through phenomenography. Library and Information Research, 36(112), 96-119. https://doi.org/10.29173/lirg496
- Zhang, N., Huang, H., Su, B., Zhao, J., & Zhang, B. (2014). Information dissemination analysis of different media towards the application for disaster pre-warning. PLoS One, 9(5), 1-12. https://doi.org/10.1371/journal.pone.0098649
- Zimmerman, M. S. (2021). Health information-seeking behavior in the time of COVID-19: information horizons methodology to decipher source path during a global pandemic. ournal of Documentation, 77(6), 1248-1264. https://doi.org/10.1108/JD-01-2021-0022
How to cite this paper
Appendices
Appendix 1: Good information experiences
| Theme | Respondents’ Comments |
|---|---|
| Factual information (26.2%) | ‘Good experiences involve reading something that seems to stick to facts without hype and things that avoid using linguistic terms designed to manipulate emotions or beliefs’. ‘Excellent news updates from Poynter, Buzzfeed, Misinfocon regarding specific trends in misinformation/fraud/hacking surrounding the pandemic; foreign news sources, WHO and some CDC sources have been valuable’ |
| Information about collective well-being (22.1%) | ‘I've seen a couple of stories about folks who had survived other diseases, the Holocaust, and now COVID-19. It shows the resiliency of the human spirit’. ‘People sharing ways of coping, for example, recipes or free yoga and meditation classes. People sharing information that helps me keep myself and my family safe. For example, how to clean produce, how to clean surfaces, how to shop for groceries etc’. |
| State government & local news information (18.2%) | ‘Good experience is when my local government puts information on their social media accounts so I can easily access it’. ‘A good experience was the governor's televised announcements’. |
| Information about leisure & social activities (5.6%) | ‘A trio of friends agreed to exchange poems every day, which means 1) I know they're still alive; 2) I've been introduced to poems by Mary Jo Salter, Stevie Smith, et al., and 3) Zoom and e-mail contacts with friends and family’. ‘Having the opportunity for more flexibility in my day - being able to be outside more, more time with my pets and spouse. Really trying to focus on the bright side of things and being vocal about it’. |
| Information from Dr. Fauci (2.5%) | ‘Dr. Fauci is the greatest example of good experiences’. ‘I love rallying around science, like Dr. Fauci. It makes me feel like my college education is something to be proud of and not something being ridiculed by the Right’. |
| Information coming from President Trump & his administration (0.3%) | ‘President Trump's daily briefings are very helpful, and he is allowing industries to step up and meet public needs’. ‘NPR consistently qualifying statements from President Trump with information from actual public health experts’. |
Appendix 2: Bad information experiences
| Theme | Respondents’ Comments |
|---|---|
| Misinformation, fake news, and conspiracy theories (27%) | ‘My friend sharing fake news with me and my husband (who gets much of his info from Facebook) telling me about virus conspiracy theories or showing me videos of people dying or bodies in churches’. ‘‘Friends sharing the Plandemic video or other Youtube viedos from "medical" experts filled with bad information’. |
| Information coming from Trump & his administration (18.2%) | ‘I can't believe I'm saying this, because it's not typically true for me, but I cannot listen to our current President's briefings. They're toxic, sound uninformed, and get my blood pressure up.” ‘Negative would be any time I tune in to see Trump's daily briefings, which are filled with bad information and dangerous information’. |
| Politics of information (11%) | ‘Seeing surprising and sometimes almost nonsensical views and advice emanating from some of the most highly placed officials in the country’. ‘Bad experiences include any information shared by people who have never worked a day in public health that think they know best and biased news stations, like FOX news, that is always blaming the other party for a global pandemic’. |
| Health-related information (10.8%) | `I also was very shocked to see an article from my hometown paper on Facebook Announcing Covid cases very close to me.” ‘Some examples of bad experiences are when I have noticed myself getting panicky after reading stories that seem unnaturally alarmist or fit my situation too closely--like when you hear about someone your exact age with your exact health conditions dying of the virus, etc’. |
| Contradictory information (5.3%) | ‘The mask controversy has been aggravating - we KNOW they could have helped earlier’. ‘The rush of sometimes contradictory information about the virus can be overwhelming and scary. My governor isn’t always clear about stay-at-home orders, and it’s hard to tell if we’re in a stay-at-home order or not, when it starts/ends, what’s essential business, etc’. |
| Unknown information (2.4%) | ‘Bad experiences would include sources stating we will never get back to normal--makes me feel like I will never go back to work’. ‘Turns out some of what I'm not seeing in the news is missing because the data isn't available: Of the something like half a million U.S. residents who have been found to have COVID-19, how many have recovered? The news reporting on numbers generally omits mention of recoveries, apparently because nobody has been counting. This could lead to the impression that nobody ever records. And I still have questions about transmission methods; the likelihood of getting infected this way or that. Again, it appears that research results are lacking’. |
| Isolation (2.2%) | `‘My kids are getting lazy and playing too many video games! I was starting to gain weight from not moving as much’! ‘I miss my students and colleagues very much’. |
| Negative information (0.3%) | ‘Bad examples are when the media just kept reporting negative information such as the lack of supplies which threw people into a panic’. ‘Facebook, I consider to be negative information’. |
| State government and local news information (0.2%) | ‘At the state level in NH, reopening has moved too fast, with little notice and no clear consultation with the businesses it affects in our communities’. ‘Bad Experiences: Seeing Andrew Cuomo on TV constantly and his attitude’. |
Appendix 3: Notable information experiences
| Theme | Respondents’ Comments |
|---|---|
| Positive outlook on information (17.1%) | ‘Finding the rare--but fascinating--articles about the science behind the virus are very empowering for me. Simply being able to set aside the worry, fear, and day-to-day anxiety, and focus on the biology and virology of SARS-CoV-2 as a learning experience is emancipating’. ‘A silver lining has been that the majority of our community has a newfound "respect" for health information’. |
| Information uncertainty (10.1%) | ‘There is a lack of information about what test results actually mean (positive, negative, negative but a carrier). Initially, there was not a lot of information out about the number of people that survived/recovered. There is also a lack of information in my area that includes private labs doing testing’. ‘The information changes fast, because this is all new territory, and we are learning as we go. We have to adapt with the changes to be safe. Some people will be wilfully ignorant no matter what. These people are scary and can cause a lot of danger and harm to the rest of us’. |
| Politics of information (8.8%) | ‘No one is in charge. It's mayhem. We thought the Fake News era ushered in by Trump was bad. Now we're paying for it big time. No one trusts anyone anymore. Thank you for letting me vent. I hope you can find my cranky responses useful’. ‘The information coming out of the US is exposing the broken structures of our system -- capitalism, racism, ageism...etc’. |
| Coronaphobia (6.3%) | ‘It’s a dangerous virus and should be taken very seriously’. ‘Our grocery store set up a special hour for senior citizens, but it was a disaster rather than a blessing because too many people showed up and did not stay 6 feet apart’. |
| Information overload (4.5%) | ‘It’s just so much, and so devastating. Information overload can certainly be overwhelming and contribute to feelings of sadness, which are heightened because of the social isolation we’re all experiencing. I’m glad we have so many avenues of information to stay informed, prepared, and safe, but it also shows the dark side of humanity, and all the negative information takes its toll’. ‘I'm somewhat addicted to finding out the latest headlines’. |
| Depressed by situation (1.8%) | ‘Unwilling to go out, loneliness and feelings of depression’. ‘Can’t watch or listen to the news, too depressing’. |
| Social media information challenge (1.1%) | ‘Social media is both a blessing and a curse. I am so grateful to know what my loved ones are doing yet I see a lot of bad information flowing past’. ‘The flood of information that filled the news channels, social media, and all my conversations is amazing. The moment-to-moment changes as more was learned about the virus was exciting to see but also challenging to take in and process. The ability to learn, change, cope, and overcome is astounding in the human brain’. |
| Denial about COVID-19 (0.8%) | ‘Friend's son collapsed and went into cardiac arrest. He had blood clots in his lungs. Family still is in denial about Covid19’. ‘People believing it is a hoax’. |
| Angered by situation (0.6%) | ‘It's horrible for my children to be out of school for this long, especially where we live’. ‘Seeing other states live freely while we are locked down and doing our part is disheartening and angering’. |
Appendix 4: Survey Questions
- Birth year (YYYY, e.g., 1991)
- What is your gender?
- Female
- Male
- Transgender, Nonbinary, or
- Other
- City, state
- Are you (Please check all that apply):
- Student (Undergraduate, graduate, Ph.D.)
- Employed
- Self-employed
- Unemployed
- Homemaker
- Retired
- Veteran
- Other (Please specify):
- In which language(s) do you search for or receive information?
- English
- Spanish
- Others (Please specify):
- Do you belong to a group that is at high risk due to coronavirus?
- Yes
- No
- Don’t know
- Have you or someone in your immediate environment been diagnosed with coronavirus?
- Yes
- No
- Don’t know
- Where do you get coronavirus information/news at the moment? How many times a day you seek coronavirus information/news? How do you stay updated about the situation? For example: Centers for Disease Control and Prevention (CDC), Federal Emergency Management Agency (FEMA), government health services websites, a cable news channel (e.g., CNN, Fox, etc.) on television and/or radio, websites, newspapers, friends, relatives, or social media (e.g., Facebook, Instagram, YouTube, WhatsApp, Snapchat, TikTok, etc.).
- Why do you choose these sources to get coronavirus information/news?
- Do you consider false or unreliable information about the pandemic to be a problem for you (for example, rumors, misunderstandings, misleading information/disinformation, or contradicting information)? In what way is it a problem?
- How do you evaluate the reliability of the information or news you receive?
- How do you cope with the amount of information/news you receive (e.g., too much information, too little information)? What kinds of feelings do you have about the amount of information (e.g., cranky, scared)?
- Please share 1-2 examples of good experiences and 1-2 examples of bad experiences that you’ve had regarding information about the coronavirus pandemic.
- Please share any other notable experiences regarding coronavirus information in general.